What if I told you there’s an even better method for lab interpretation than functional blood chemistry analysis?
One where the results are more accurate, research-based, and personalized to each patient?
And that your patients—and your business—can benefit with no gimmicks, sleazy sales techniques, or an MLM to join?
We’ve all experienced the excitement of learning about and applying functional reference ranges.
Functional blood chemistry analysis has helped us unlock seemingly unsolvable health mysteries and support our sickest patients.
It’s an incredible tool. But there’s something better.
History of functional blood chemistry analysis
“Optimum” reference ranges were initially defined in 1994 by Dr. Harry O. Eidenier, Sr., the godfather of functional blood chemistry analysis, based on data gathered as far back as 1980 on approximately 10,000 people.
Dr. Eidenier and his colleagues combined blood test results with physical exams, health histories, and other assessments such as stool and hair mineral analyses in what he called the “Biochemical Biopsy.”
This data resulted in a set of reference ranges that have been used as the functional blood chemistry analysis standard for many years.
But even Dr. Eidenier stated that his findings were not absolute and were primarily based on empirical evidence.
Building on the functional blood chemistry analysis legacy
Unfortunately, two critical sources of information were missing from the criteria used to develop functional ranges:
- The results of peer-reviewed hematological studies
- Individual influences shown in the research literature to affect blood test results, such as:
- Age
- Sex
- Ethnicity
- Pregnancy (by trimester)
- Menopausal status
- Menstrual phase
- Elevation (altitude)
- Alcohol intake
- Smoking status
The results of test interpretations change drastically when these factors are included in functional blood chemistry analysis.
These same results heavily influence your course of treatment and, ultimately, your patient’s results.
Where do we go from here…
Bio-individual Blood Chemistry Analysis
Currently, neither conventional laboratory ranges nor those used in functional blood chemistry analysis account for personal influences.
Biological traits of individuals can have an impact on the expected “normal” reference range.
Adjusting for these factors is what makes Bio-individual Blood Chemistry Analysis more accurate than functional blood chemistry analysis!
Below is a small sample of studies exploring the clinically significant influences of age, sex, pregnancy, smoking status, menopausal status, ethnicity, elevation, alcohol intake, and menstrual phase on blood test results.
Age and Sex
- A population-controlled study of over 40,000 people by Fulgoni et al., 2019 found that males versus females and younger versus older people had clinically significant differences in red blood cell counts, hematocrit, and hemoglobin compared to reference ranges used in functional blood chemistry analysis.
- In a study of over 3,000 people (~half males and half females) by Ittermann et al., 2019, females were found to have a clinically significant increase in platelet count compared to males.
- In this same study, platelet counts were inversely associated with mean platelet volume (MPV). Heightened female platelets and the correlation with MPV are not reflected in functional blood chemistry analysis. LabSmarts also adjusts platelet reference ranges based on MPV!
Pregnancy and Menstrual Phase
- Physiological anemia, also called “dilutional anemia,” may occur during the second (luteal) phase of the menstrual cycle and pregnancy due to the actions of relaxin and a relative increase in plasma volume.
- Dilutional anemia is a normal occurrence and should not be treated as pathological anemia. However, this allowance is not considered in functional blood chemistry analysis.
- Sullivan et al., 2008 suggest that decreases in hemoglobin during each pregnancy trimester should be accounted for in conventional lab ranges. Functional blood chemistry analysis does not yet account for this decrease.
Smoking
- Bilirubin levels may be reduced in active smokers, according to Zucker et al., 2004, possibly due to smoking’s effect on zinc status and oxidative stress levels.
- This influence is particularly important considering bilirubin’s paradoxical role as both endogenous antioxidant and possible toxin.
- According to Malenica et al., 2017, those who smoke tobacco had significant increases in white blood cells, hemoglobin, mean corpuscular volume, and mean corpuscular hemoglobin concentrations.
- Further, male smokers had higher levels of red blood cells, white blood cells, hemoglobin, hematocrit, and mean corpuscular hemoglobin compared to female smokers.
- Functional blood chemistry analysis does not account for these smoking-dependent changes.
Elevation (altitude)
- Elevation is a well-known influence on blood test outcomes that affects over six million people in the United States.
- After approximately two weeks, clinically significant increases in hemoglobin occur at elevations over about 3,280 feet.
- However, functional interpretation does not account for this increase.
Remember, studies exploring menopausal status, ethnicity, and alcohol intake also reveal that these factors influence blood test results.

Incorporating Bio-individual Blood Chemistry Analysis into your practice
Consider a new female patient who is in the luteal, high-hormone phase of her menstrual cycle, lives in Denver, Colorado, and is a long-distance runner.
She presents with complaints of extremely low energy and bloating. But her periods are normal—no heavy bleeding—and she doesn’t have any other significant health issues.
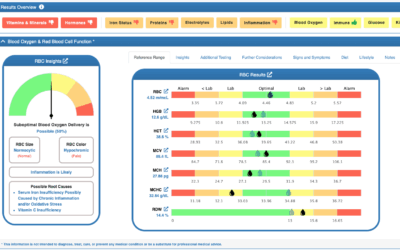
Her red blood cell count, hemoglobin, and hematocrit levels are at the low end of the optimal range, and her mean corpuscular volume, mean corpuscular hemoglobin, and mean corpuscular hemoglobin concentration are optimal.
Based on your knowledge of functional blood chemistry analysis, since all of these values are in the optimal range, you don’t consider anemia as a cause of her severe fatigue.
So, if it’s not anemia, what might be happening?
If functional blood chemistry analysis factored in her elevation (5,277 feet) like LabSmarts does, her reference ranges would shift upward to account for her high elevation, and her RBC, HGB, and HCT values would now be below optimal. This pattern is now a normocytic normochromic type of anemia.
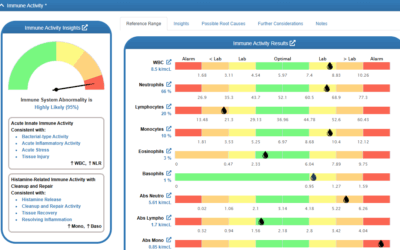
You’d look at other markers and notice that her total bilirubin is elevated which can indicate premature RBC destruction. LabSmarts automatically identifies this as a possible root cause of her anemia based on this pattern.
You also learn from LabSmarts that “footstrike hemolysis” can be a possible root cause of premature RBC destruction and you correlate that with her long distance running.
Your patients’ or clients’ bio-individual factors directly impact the accuracy of your blood test interpretation, treatment plan, and health outcomes.
As shown above, the research is out there—now we need to apply it.
If you’re a research buff, investigate your patients’ individual factors and how they impact blood test outcomes.
- What is your patient’s age and sex?
- Is your patient pregnant? And if so, what trimester are they currently in?
- Do they live at an elevation above approximately 3,300 feet?
- Do they frequently consume alcohol? Do they smoke?
- Are they menopausal?
- Where are they in their menstrual cycle?
- What is their ethnicity?
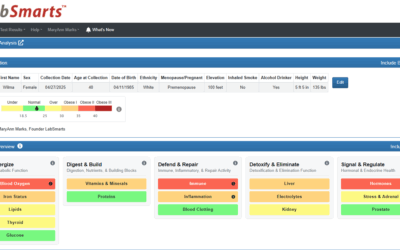
Or, instead of doing all of this research yourself, you’re welcome to sign up for a free trial of LabSmarts, the only research-based, bio-individual blood chemistry analysis software available!
Our software considers all of the personalized elements discussed in this blog and, thanks to colorful automated reports, it makes the findings easy (and attractive) to explain to patients. And we’re constantly updating our research based on new findings so you’re ahead of the curve.